Image Formalizing how plants live and adapt through algorithms April 30, 2025 From exploring plant phenomics to developing 3D images of plants, Dr. Alexander Bucksch is reimagining how we study them to revolutionize agriculture. Read more
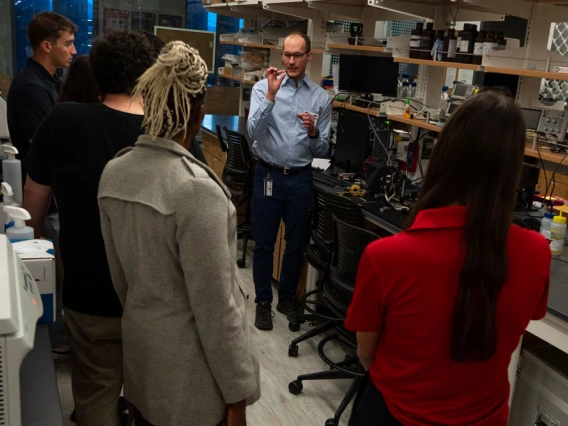
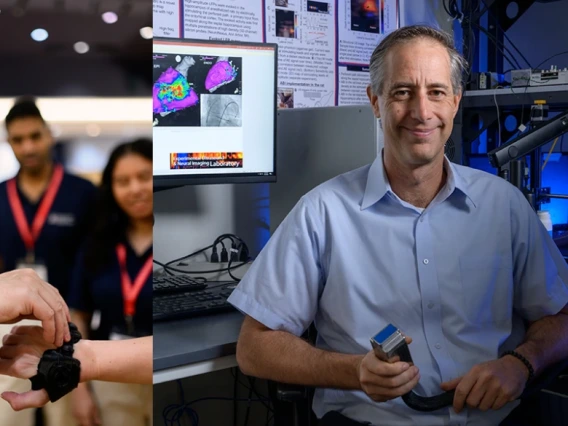
Image Community members go behind-the-scenes at the BIO5 Institute April 22, 2025 Guests experienced the collaborative nature of research through conversations, hands-on demos, and real-world applications at the annual public event. Read more
Image Meet the scientists Behind BIO5 April 22, 2025 At an annual community event in early April, attendees heard from five accomplished University of Arizona researchers from diverse scientific disciplines during a series of intimate fireside chats. Read snapshots of these conversations. Read more
Image A tale of two cities and a health mystery April 16, 2025 Multiple BIO5 members lead the BEAMS study, investigating how early-life environmental exposures across the U.S.-Mexico border impact asthma risk. Read more in U of A Health Sciences
Image Researchers launch startup to bring novel treatments to patients with asthma and COPD April 16, 2025 BIO5 Members Julie Ledford, Josef Vagner, Stefano Guerra, and Michael D.L. Johnson co-developed an innovative inhaled asthma/COPD therapy licensed to Aspiro Therapeutics. Read more in U of A Health Sciences
Image From engineering dreams to virology breakthroughs April 15, 2025 Dr. Pierce Longmire is a molecular virologist passionate about studying pathogens and sharing his science with the community. Read more
Image Waking up to the interdisciplinary science of sleep April 14, 2025 2025 BIO5 Postdoctoral Fellow Kat Kennedy blends an interdisciplinary background to explore how sleep affects health, cognition, and society. Read more
Image Biomedical engineering faculty win grants to advance research to market April 3, 2025 BIO5 members Zong-Ming Li and Russell Witte received 2025 Flinn Foundation seed grants for their innovative work. Read more in U of A College of Engineering
Image Connecting with Frederic Zenhausern, PhD March 31, 2025 BIO5 member Frederic Zenhausern leads the Center for Applied NanoBioscience and Medicine, uniting research from molecular science to space exploration. Read more in U of A Health Sciences
Image Four U of A professors named AAAS fellows March 28, 2025 BIO5 members Luciano Matzkin, Armin Sorooshian and Jil Tardiff, have been elected fellows of the American Association for the Advancement of Science. Read more in U of A News